Lancet子刊 | 新联合方案治疗复发性神经母细胞瘤显疗效
神经母细胞瘤是儿童中最常见的颅外实体肿瘤。约25%的神经母细胞瘤中存在MYCN扩增,这通常预示着较差的预后。高危神经母细胞瘤患者即使接受了强化的多模式治疗仍有超过一半的患者会在诊断后两年内复发。此外,10-20%的患者对一线化疗显示耐药性。对于复发性高危神经母细胞瘤患者,其4年无进展生存率和总生存率仅分别为6%和20%,而中位无进展生存期仅为6.4个月,这凸显了高危神经母细胞瘤作为儿童癌症中最为严峻疾病之一的挑战性。
尽管预后挑战巨大,但研究表明, 伊立替康(Irinotecan)和替莫唑胺(temozolomide)在复发性和难治性神经母细胞瘤中显示出疗效;此外,mTOR信号通路在神经母细胞瘤中具有重要作用。 临床前研究中,mTOR抑制剂雷帕霉素(rapamycin)与酪氨酸激酶(tyrosine kinase)抑制剂协同作用显著,能诱导放射增敏和化疗增敏。这种效果在MYCN扩增的神经母细胞瘤中尤其突出,为后续临床研究奠定了基础。
近日,由 Dr Selim Corbacioglu 团队发表于 Lancet Oncology 题为 Irinotecan and temozolomide in combination with dasatinib and rapamycin versus irinotecan and temozolomide for patients with relapsed or refractory neuroblastoma (RIST-rNB-2011): a multicentre, open-label, randomised, controlled, phase 2 trial 的文章, 首次探索了代谢节律性、途径导向的四药联合疗法的疗效,这项二期临床试验RIST-rNB-2011显示,雷帕霉素-达沙替尼联合伊立替康-替莫唑胺可显著延长MYCN扩增型复发性神经母细胞瘤患者的无进展生存期(PFS)和总体生存期(OS),同时具有良好的耐受性。这一发现也为RIST方案成为潜在的一线治疗方案提供了可能。
RIST-rNB-2011是一项在德国和奥地利的40家儿童肿瘤中心进行的II期临床试验。从2013年到2020年招募的对象包括1至25岁的儿童、青少年和年轻成人(Lansky或Karnofsky体能评分至少50%)。这些患者均为高危(国际神经母细胞瘤分期系统[INSS] IV期病灶或所有MYCN扩增分期)复发(定义为治疗后出现复发,包括多次复发,且不限制既往治疗)神经母细胞瘤患者,已接受强化的多模式高危治疗,或为耐药性神经母细胞瘤患者(初始治疗期间病情进展)。
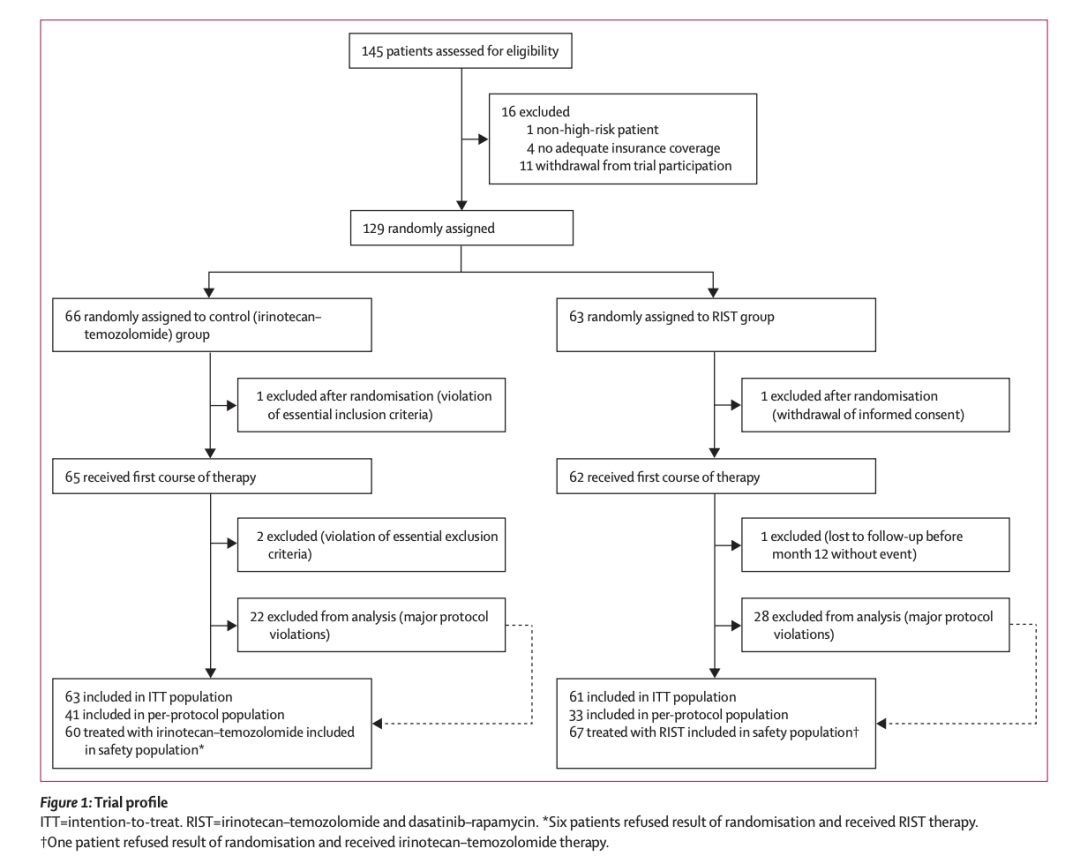
本试验一共招募了129名患者;他们被随机1:1分配至RIST组或伊立替康-替莫唑胺(对照组)并确保 各组中 MYCN扩增患者均匀分布 。(详情见图一)
RIST组治疗方案 由雷帕霉素-达沙替尼疗程和伊立替康-替莫唑胺疗程交替组成,总疗程为20周。
雷帕霉素-达沙替尼疗程 中,患者第1天接受口服雷帕霉素的负荷剂量(3 mg/m²),随后在第2至第4天调整为维持剂量(1 mg/m²),同时每日口服达沙替尼(2 mg/kg,最大剂量140 mg/天),持续4天后停药3天。在第5天通过血清检测监测雷帕霉素浓度,并调整后续疗程的剂量至3–10 ng/mL范围,以确保治疗的稳定性和有效性。
伊立替康-替莫唑胺疗程 包括每日口服替莫唑胺(150 mg/m²)和静脉注射伊立替康(50 mg/m²),连续5天后停药2天,以完成一个疗程。
-
第一阶段(8周) :包括4个周期,每个周期由1个雷帕霉素-达沙替尼疗程和1个伊立替康-替莫唑胺疗程组成。
-
第二阶段(12周) :包括4个周期,但每周期调整为2个雷帕霉素-达沙替尼疗程和1个伊立替康-替莫唑胺疗程,以增加靶向治疗的比例。
第二阶段的设计旨在减少化疗相关毒性,例如血液系统损伤,从而避免治疗延迟,并为患者提供更充足的血液系统恢复时间。同时,通过持续使用靶向药物维持对癌细胞的抑制作用。这种代谢节律性方案确保了治疗的有效性,同时最大限度地减少了不良反应的发生。
本次试验主要终点是无进展生存期(PFS),次要终点包括总体生存期(OS)。
本次试验结果如下:
-
-
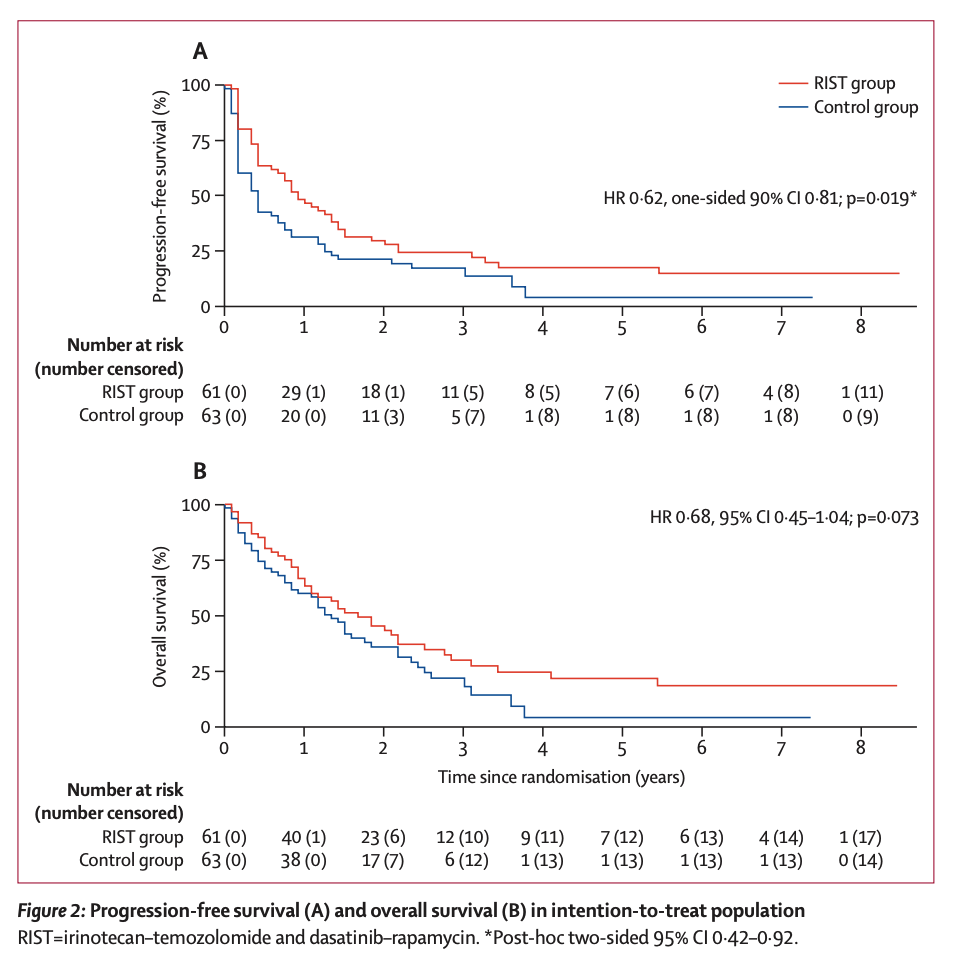
RIST组(n=49)的中位无进展生存期为11个月(95% CI 7–17),对照组(n=54) 为5个月(2–8)(HR 0.62,p=0.019)。(见图二A)
-
MYCN扩增患者中 ,RIST组的中位PFS显著长于对照组(6个月 vs 2个月,p=0.012)。
-
非MYCN扩增患者中 ,RIST组与对照组差异不显著(14个月 vs 8个月,p=0.49)。
-
-
RIST组的中位总体生存期为20个月(95% CI 13–30),对照组为16个月(10–22),但未达到统计学显著性(p=0.073)。
-
-
基于医生决策的单倍体造血干细胞移植中, MYCN扩增患者在RIST组的生存率更高(83% vs 0%)。这可能归因于RIST治疗帮助患者实现了**最小残留病灶(MRD)**状态,从而允许更持久的细胞巩固治疗。
-
-
RIST组的毒性反应与对照组相似,未发现显著差异。
因此,RIST治疗显著改善了无进展生存期(PFS),并使复发或难治性神经母细胞瘤患者的总体生存期(OS)明显延长(虽然未达到统计学显著性)。 并且RIST的协同作用在MYCN扩增的肿瘤和细胞系中尤为显著。
本试验也探究为什么MYCN扩增患者在接受RIST治疗和单倍体造血干细胞移植后生存率更高; 这可能是因为这些患者达到了最小残留病灶(MRD)状态,从而能够进行持久的细胞巩固治疗。因此,RIST治疗能够在MYCN扩增的复发或难治性神经母细胞瘤患者中诱导缓解,并实现持续的无进展生存。 因此未来试验需要进一步确定最适合的巩固治疗方案。 所以RIST试验的结果为MYCN扩增型神经母细胞瘤患者在一线治疗中采用类似RIST的治疗方案提供了新的讨论方向。
即使本试验仍然存在局限性(招募周期较长,符合方案人群样本少,观察到的毒性反应导致方案违背几乎完全于与伊立替康-替莫唑胺),但是RIST试验首次表明, 在MYCN扩增型复发或难治性神经母细胞瘤患者中,雷帕霉素-达沙替尼联合伊立替康-替莫唑胺能够改善长期的无进展生存期(PFS)和总体生存期(OS),证明了MYCN扩增是一个具有临床相关性的分子靶点。 本研究中使用的药物普遍可及,多数为口服液制剂,且适用于门诊治疗,同时具有可接受的不良事件特征,这表明RIST方案可能成为最脆弱的神经母细胞瘤患者的一种潜在治疗选择。
撰文
责编
制作
排版 | 车洁 校对 | uu
▼滑动查看更多▼
Background: Neuroblastoma is the most common extracranial solid tumour in children. Relapsed or refractory neuroblastoma is associated with a poor outcome. We assessed the combination of irinotecan-temozolomide and dasatinib-rapamycin (RIST) in patients with relapsed or refractory neuroblastoma.
Methods: The multicentre, open-label, randomised, controlled, phase 2, RIST-rNB-2011 trial recruited from 40 paediatric oncology centres in Germany and Austria. Patients aged 1-25 years with high-risk relapsed (defined as recurrence of all stage IV and MYCN amplification stages, after response to treatment) or refractory (progressive disease during primary treatment) neuroblastoma, with Lansky and Karnofsky performance status at least 50%, were assigned (1:1) to RIST (RIST group) or irinotecan-temozolomide (control group) by block randomisation, stratified by MYCN status. We compared RIST (oral rapamycin [loading 3 mg/m2 on day 1, maintenance 1 mg/m2 on days 2-4] and oral dasatinib [2 mg/kg per day] for 4 days with 3 days off, followed by intravenous irinotecan [50 mg/m2 per day] and oral temozolomide [150 mg/m2 per day] for 5 days with 2 days off; one course each of rapamycin-dasatinib and irinotecan-temozolomide for four cycles over 8 weeks, then two courses of rapamycin-dasatinib followed by one course of irinotecan-temozolomide for 12 weeks) with irinotecan-temozolomide alone (with identical dosing as experimental group). The primary endpoint of progression-free survival was analysed in all eligible patients who received at least one course of therapy. The safety population consisted of all patients who received at least one course of therapy and had at least one post-baseline safety assessment. This trial is registered at ClinicalTrials.gov, NCT01467986, and is closed to accrual.
Findings: Between Aug 26, 2013, and Sept 21, 2020, 129 patients were randomly assigned to the RIST group (n=63) or control group (n=66). Median age was 5·4 years (IQR 3·7-8·1). 124 patients (78 [63%] male and 46 [37%] female) were included in the efficacy analysis. At a median follow-up of 72 months (IQR 31-88), the median progression-free survival was 11 months (95% CI 7-17) in the RIST group and 5 months (2-8) in the control group (hazard ratio 0·62, one-sided 90% CI 0·81; p=0·019). Median progression-free survival in patients with amplified MYCN (n=48) was 6 months (95% CI 4-24) in the RIST group versus 2 months (2-5) in the control group (HR 0·45 [95% CI 0·24-0·84], p=0·012); median progression-free survival in patients without amplified MYCN (n=76) was 14 months (95% CI 9-7) in the RIST group versus 8 months (4-15) in the control group (HR 0·84 [95% CI 0·51-1·38], p=0·49). The most common grade 3 or worse adverse events were neutropenia (54 [81%] of 67 patients given RIST vs 49 [82%] of 60 patients given control), thrombocytopenia (45 [67%] vs 41 [68%]), and anaemia (39 [58%] vs 38 [63%]). Nine serious treatment-related adverse events were reported (five patients given control and four patients given RIST). There were no treatment-related deaths in the control group and one in the RIST group (multiorgan failure).
Interpretation: RIST-rNB-2011 demonstrated that targeting of MYCN-amplified relapsed or refractory neuroblastoma with a pathway-directed metronomic combination of a multkinase inhibitor and an mTOR inhibitor can improve progression-free survival and overall survival. This exclusive efficacy in MYCN-amplified, relapsed neuroblastoma warrants further investigation in the first-line setting.
Funding: Deutsche Krebshilfe.
DOI: 10.1016/S1470-2045(24)00202-X
版权声明:本文为“乐问号”作者或机构在乐问医学上传并发布,仅代表该作者或机构观点,不代表乐问医学的观点或立场,不能作为个体诊疗依据,如有不适,请结合自身情况寻求医生的针对性治疗。
链接:http://www.lewenyixue.com/2024/12/20/Lancet%E5%AD%90%E5%88%8A%20%7C%20%E6%96%B0%E8%81%94%E5%90%88%E6%96%B9%E6%A1%88%E6%B2%BB%E7%96%97%E5%A4%8D%E5%8F%91/
THE END