Lancet 子刊 | 高温天气与儿童急性淋巴细胞白血病风险相关性研究
全球气候变化背景之下,高温天气越来越常见,对人类健康和生活质量的影响也备受关注。特别是对孕妇而言,孕期暴露于高温环境可能会对胎儿的健康产生负面影响,儿童急性淋巴细胞白血病(ALL)起源于产前,被怀疑是一种潜在的不良后果。但孕期暴露于高温环境与婴儿长期健康的研究较少,因此尚未有统计学数据直接证明这一结论。
近日,来自耶鲁大学、加利福尼亚大学伯克利分校等多所高校的研究人员在 The Lancet Planetary Health 上发表题为 High ambient temperature in pregnancy and risk of childhood acute lymphoblastic leukaemia: an observational study 的文章,分析了31万份样本后指出, 孕早期暴露于高温环境(特别是在妊娠第8周左右)与儿童ALL风险增加有关。

研究人员分析了1982年1月1日~2015年12月31日期间在加利福利亚州出生的儿童数据,选取了6258份患癌儿童(在1988~2015年期间被诊断出ALL)样本和307579份对照组样本。研究人员对孕妇居住地址进行地理编码,并估算当地每日的平均温度,尽可能完整地收集到其他相关变量(如空气湿度、PM2.5等)数据以描述研究人群和控制潜在混杂因素。
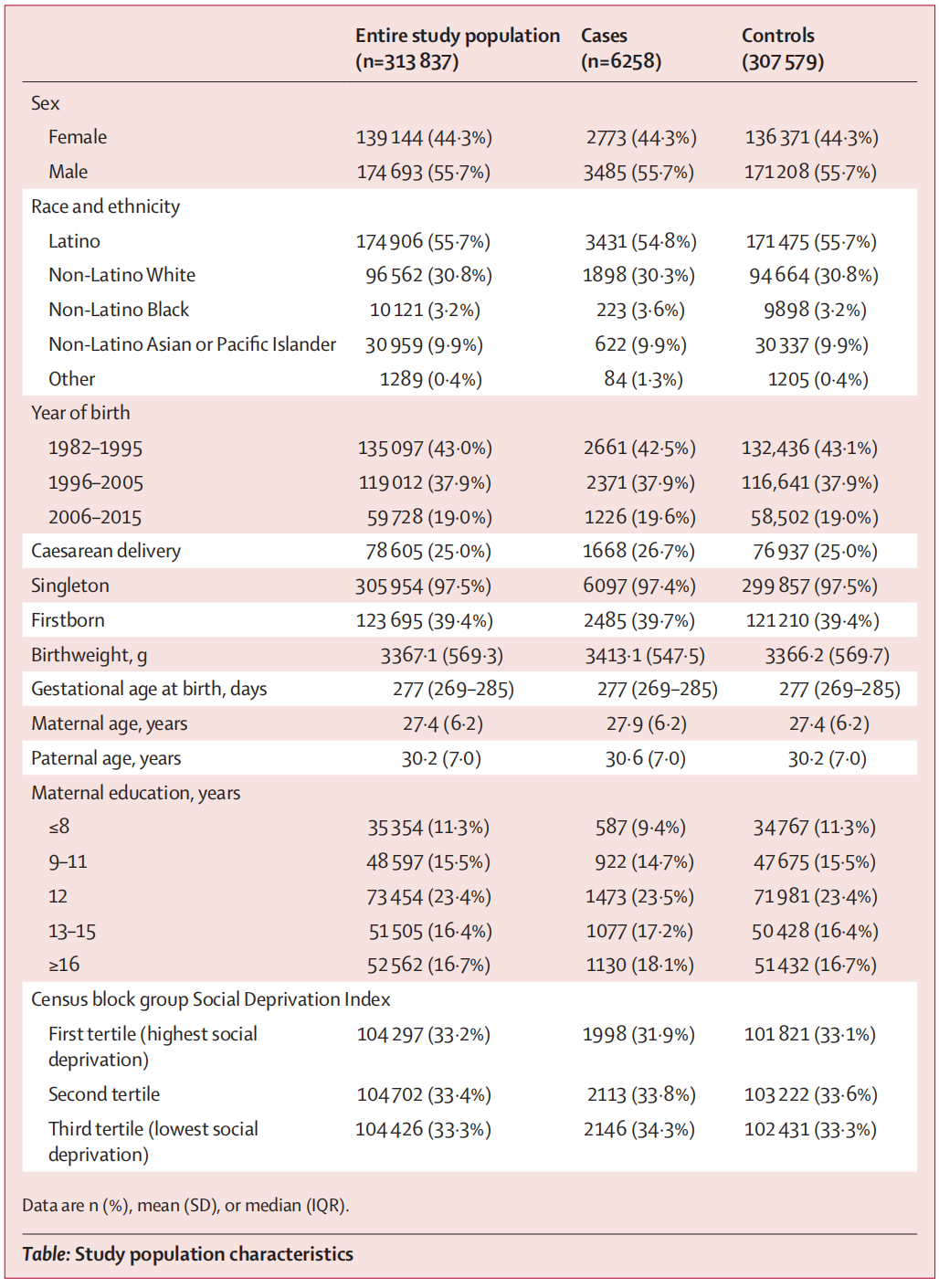
图: 313837份数据中大多数为男性(174693例,占55.7%)和拉丁裔(174906例,占55.7%),在6258例病例中,3636例(58.1%)在5岁前被诊断,1769例(28.3%)在5~9岁之间被诊断,853例(13.6%)在10~14岁之间被诊断。
统计分析结果显示,从末次月经前2周开始到妊娠第20周,高环境温度与儿童急性淋巴细胞白血病之间都存在显著关联。 在妊娠第8周时,环境温度与儿童ALL风险的关联最强 ,此时平均每周温度升高5°C,ALL的优势比为1.07(95%CI 1.04 - 1.11)。
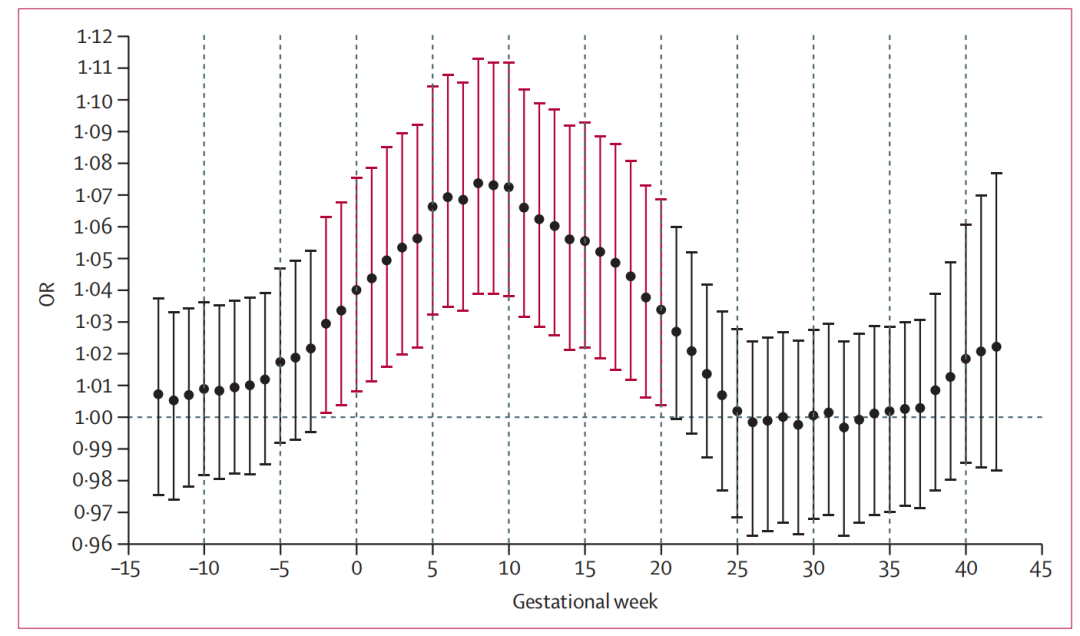
图:孕周数与优势比(OR,odds ratio)的曲线图。红色线条表述高环境温度与儿童急性淋巴细胞白血病发生率显著相关。(OR是流行病学和统计学中常用的一个指标,用于衡量某个因素与事件发生之间的关联强度)
拉丁裔儿童在妊娠第8周时受高温影响的优势比为1.09(95%CI 1.04 - 1.14),非拉丁裔白人儿童为1.05(95%CI1.00 - 1.11),虽然相对来说拉丁裔儿童受高温影响的关联性更高,但统计数据并不具显著性(p = 0.24)。此外, ALL诊断年龄在0 - 4岁和5 - 9岁的儿童与其母亲孕期暴露于高温环境的关联较为明显,而10 - 14岁诊断的儿童与温度无关联。
值得注意的是,较高的空气污染水平下, 高环境温度暴露与急性淋巴细胞白血病风险之间的正相关更为显著。
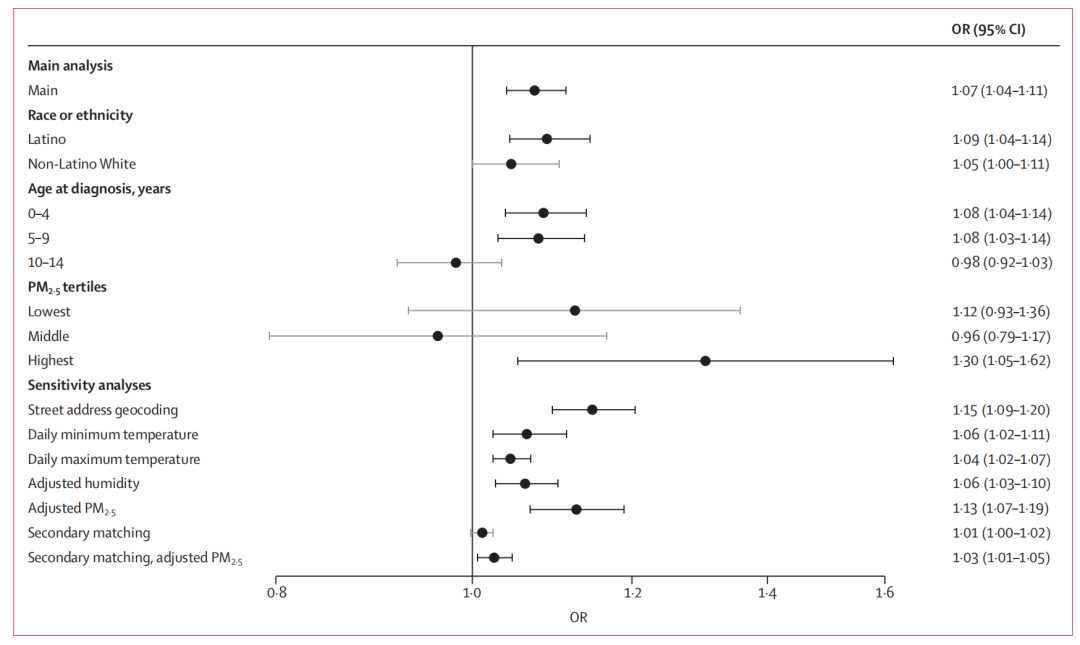
图:民族、年龄与空气污染物等其他因素与儿童急性淋巴白血病之间的关联性
本次研究并未直接揭露孕期高温暴露与儿童ALL关联性的生物学机制,但由于检测到患儿在出生时就存在白血病前期克隆,且孕期第8周与儿童ALL关联性最强,研究者们认为孕早期最有可能是关键窗口期。 研究略有瑕疵之处在于,样本数据可能存在固定队列偏差和活产偏差,个体对高温的暴露也未考虑到空调使用、工作类型等因素的影响(对结果的影响不会有大的偏差)。
尽管如此,该研究仍具有重要的社会学和医学意义。它 首次建立了孕期暴露于高温环境与儿童ALL风险之间的稳健关联 ,强调了高温环境不仅对人类健康有即时影响,还可能对下一代儿童的健康造成负面影响。对于医疗工作者、患者和患者家属来说,这些发现有助于提高对孕期环境因素的重视,为预防和治疗儿童ALL提供新的思路。
撰文
责编
制作
排版 | 车洁 校对 | uu
▼滑动查看更多▼
Background
High ambient temperature is increasingly common due to climate change and is associated with risk of adverse pregnancy outcomes. Acute lymphoblastic leukaemia is the most common malignancy in children, the incidence is increasing, and in the USA disproportionately affects Latino children. We aimed to investigate the potential association between high ambient temperature in pregnancy and risk of childhood acute lymphoblastic leukaemia.
Methods
We used data from California birth records (children born from Jan 1, 1982, to Dec 31, 2015) and California Cancer Registry (those diagnosed with childhood cancer in California from Jan 1, 1988, to Dec 31, 2015) to identify acute lymphoblastic leukaemia cases diagnosed in infants and children aged 14 years and younger and controls matched by sex, race, ethnicity, and date of last menstrual period. Ambient temperatures were estimated on a 1-km grid. The association between ambient temperature and acute lymphoblastic leukaemia was evaluated per gestational week, restricted to May–September, adjusting for confounders. Bayesian meta-regression was applied to identify critical exposure windows. For sensitivity analyses, we evaluated a 90-day pre-pregnancy period (assuming no direct effect before pregnancy), adjusted for relative humidity and particulate matter less than 2·5 microns in aerodynamic diameter, and constructed an alternatively matched dataset for exposure contrast by seasonality.
Findings
6849 cases of childhood acute lymphoblastic leukaemia were identified and, of these, 6258 had sufficient data for study inclusion. We also included 307 579 matched controls. Most of the study population were male (174 693 [55·7%] of the 313 837 included in the study) and of Latino ethnicity (174 906 [55·7%]). The peak association between ambient temperature and risk of acute lymphoblastic leukaemia was observed in gestational week 8, where a 5°C increase was associated with an odds ratio of 1·07 (95% CI 1·04–1·11). A slightly larger effect was seen among Latino children (OR 1·09 [95% CI 1·04–1·14]) than non-Latino White children (OR 1·05 [1·00–1·11]). The sensitivity analyses supported the results of the main analysis.
Interpretation
Our findings suggest an association between high ambient temperature in early pregnancy and risk of childhood acute lymphoblastic leukaemia. Further replication and investigation of mechanistic pathways might inform mitigation strategies.
Funding
Yale Center on Climate Change and Health, The National Center for Advancing Translational Science, National Institutes of Health.
DOI: 10.1016/S2542-5196(24)00121-9
版权声明:本文为“乐问号”作者或机构在乐问医学上传并发布,仅代表该作者或机构观点,不代表乐问医学的观点或立场,不能作为个体诊疗依据,如有不适,请结合自身情况寻求医生的针对性治疗。
链接:http://www.lewenyixue.com/2024/08/01/Lancet%20%E5%AD%90%E5%88%8A%20%7C%20%E9%AB%98%E6%B8%A9%E5%A4%A9%E6%B0%94%E4%B8%8E%E5%84%BF%E7%AB%A5%E6%80%A5/
THE END





赶快来坐沙发